
Atrial Fibrillation
Atrial Fibrillation - Cardiologist in Mildura
Atrial fibrillation is the most common heart rhythm disturbance in the world. It affects patients in all age groups – young and old (more particularly the elderly), sick and well, as well as in all kinds of clinical scenarios.
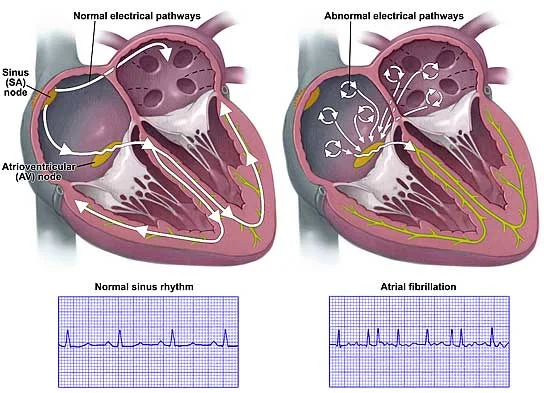
Normally the heart beats with the top chambers (atrium) contracting first, and then the electrical signals are passed down to the ventricles, which will then contract to expel the blood away from the heart. In atrial fibrillation, the top chambers are no longer pumping synchronously, and in fact are in total electrical chaos, with tiny electrical contractions all over the atria – resembling a “bag of worms”. When this happens, clot may form in the atria (top chambers), especially in the left atrial appendage. Clots flicking off during atrial fibrillation is a major cause of stroke in the elderly.
Click here to obtain a pamphlet about atrial fibrillation and its therapy.
Heart conditions – atrial fibrillation – Better Health Channel
Atrial fibrillation (AF) is a type of arrhythmia. The heart beats abnormally and this can cause palpitations or a fluttering heartbeat, irregular heartbeat, chest pains, dizziness or fainting spells. AF can remain undetected for long periods of time. Untreated, complications may include stroke and heart attack. Treatment options include medication, surgery and electric shock therapy. An artificial pacemaker may be inserted to maintain regular heart rhythm.
AF is the most commonly encountered heart rhythm disturbance in my practice. Everyday, I come across patients with either recent onset AF, chronic AF, or complications of AF, namely – congestive heart failure, breathlessness, dizziness and occasionally blackouts, and stroke.
Strategies to treat AF are broadly divided into two options –
1. Revert the AF to normal sinus rhythm (RHYTHM CONTROL), or
2. Leave the patient in AF (RATE CONTROL) but maintain a reasonable heart rate + prevent complications (stroke, heart failure).
RHYTHM CONTROL
Pharmacological cardioversion: medications can be used to revert AF to sinus rhythm: Flecainide, sotalol or amiodarone.
Electrical cardioversion is the other alternative to pharmacological cardioversion – in this case the patient undergoes electrical shock under brief general anaesthetic to revert the AF to sinus rhythm.
In all cases of cardioversion, prevention of clot formation and subsequent risk of stroke is important, usually the patient is anticoagulated with either warfarin or subcutaneous anticoagulation prior to cardioversion. In urgent cases, patient may undergo transoesophageal echocardiogram to exclude any (left atrial appendage) clots prior to electrical cardioversion.
RATE CONTROL
In this case, the atrial fibrillation is accepted as the long term heart rhythm, and the heart rate is the main item to control. Many medications are used to maintain reasonable heart rate – beta-blockers, calcium-channel blockers, digoxin to name a few. Depending on the stroke risk, the patient is also advised to take anticoagulant therapy to prevent stroke.
Prevention of stroke is one of the most important therapies of AF. One uses the CHADS2 or CHADsVASC score to determine a patient’s risk of stroke.
C = congestive heart failure (1 point)
H = hypertension (1 point)
A = age over 75 years (1 point)
D = diabetes (1 point)
S2 = prior stroke (2 points)
1 point = low risk of stroke (aspirin 100 mg daily is reasonable, or you may want to consider anticoagulation)
2 – 4 points = medium risk of stroke (Anticoagulation recommended)
5 – 6 points = high risk of stroke (Anticoagulation recommended)
NOACs (Novel Oral AntiCoagulants)
Pacemakers
In general, pacemakers do not prevent atrial fibrillation or stroke. Pacemakers are helpful when individuals develop very fast and slow heart rates. Fast heart rates are treated with medications, slow heart rate are not able to be treated with medications, as there are no medications that can speed up the heart. In this case, a pacemaker is inserted to protect against slow heart rate, whilst at the same time medications are used to treat the fast heart rates.
Occasionally AF may result in so much symptoms that it may be necessary to sever the electrical fibre connection between the top and bottom heart chambers, a procedure called atrioventricular nodal ablation (AV node ablation). After ablation (performed as a keyhole procedure), the patient should not feel the palpitations any more, but will be permanently dependent on a pacemaker (which is inserted a month or two before the ablation).
Newer techniques of cure of AF involves a procedure called pulmonary vein isolation ( ablation ). See the videos at the top of this page.
Devices (e.g. Watchman device) may sometimes be inserted into the left atrial appendage to prevent clots from lodging there. This may be an alternative to taking warfarin.